How to Prescribe Idrasil™?
Simply Write Idrasil™ 12.5 mg, 25 mg, or 100 mg PRN / Q 6H on Your Prescription Pad
6.25 : 1 : 6 Titration Rule
6.25 mg / 100 lbs / 6 hours
Fill out this document and transmit electronically by email or fax.
Fax: (855)437-2779
Email : patientservices@idrasil.com
Click to Download
Have questions? Call our 24/7 Hotline 1-855-437-2745
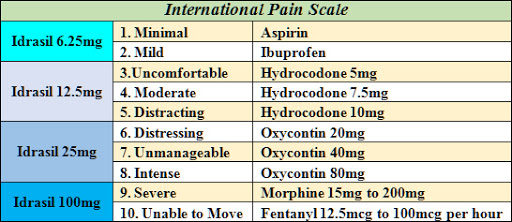
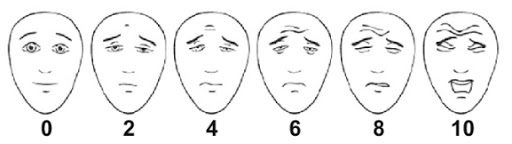
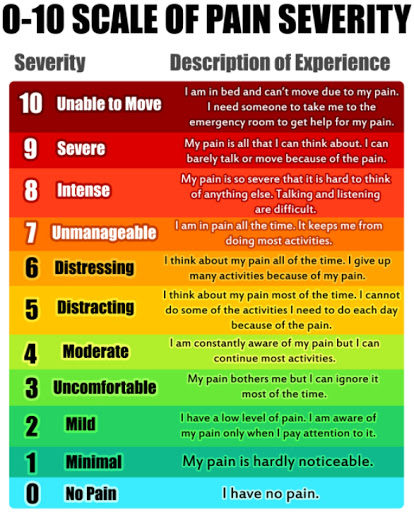
Pain Scale of Idrasil™