2737 BC: Cannabis is referred to as a “superior” herb in the world’s first medical text, or pharmacopoeia, Shen Nung’s Pen Ts’ao, in China.
1500 BC: Cannabis-smoking Scythians sweep through Europe and Asia, settling and inventing the scythe.
1400 BC: Cultural and religious use of ganga or cannabis and charas or hashish (resin) recorded used by Hindus in India.
600 BC: Zend-Avesta, Indian scripture, speaks of hemp’s intoxicating resin.
500 BC: Gautama Buddha said to have survived by eating hempseed. Cannabis used in Germany (Hochdorf Hallstatt D wagon burial site). First botanical drawings of cannabis in Constantinopolitaus.
450 BC: Herodotus records Scythians and Thracians as consuming cannabis and making fine linens of hemp.
300 BC: Carthage and Rome struggle for political and commercial power over hemp and spice trade routes in the Mediterranean.
100 BC: Chinese make paper from hemp and mulberry.
70 BC: Roman Emperor Neros’ surgeon, Dioscorides, praises cannabis for making the stoutest cords and for its’ medicinal properties.
30 AD: Jesus teaches: Not that which goeth into the mouth defileth a man; but that which cometh out of the mouth, this defileth a man (Matthew 15: 11). The Gospels refer to the New Wine and declare that it is best when the clusters are ripe.
100 AD: Roman surgeon Dioscorides names the plant cannabis sativa and describes various medicinal uses. Pliny reported of industrial uses and wrote a manua on farming hemp.
400 AD: Cannabis cultivated for the first time in the UK at Old Buckenham Mere.
500 AD: First botanical drawing of hemp in Constantinopolitaus.
600 AD: Germans, Franks & Vikings all use hemp fiber.
800 AD: Mohammed allows cannabis but forbids the use of alcohol.
1000 AD: The English word “hempe” first listed in a dictionary. Moslems produce hashish for medicine and social use.
1150 AD: Moslems use hemp to start Europe’s first paper mill. Most of the paper is made from hemp for the next 750 years, including Bibles.
1379 AD: Emir Soudan Sheikhouni of Joneima prohibits cannabis consumption amongst the poor, destroys the crops, and punishes offenders by pulling out their teeth.
1484 AD: Inquisitor Pope Innocent VIII outlaws hashish.
1494 AD: Hemp paper industry starts in England.
1545 AD: Hemp agriculture arrives in China.
1554 AD: The Spanish grow hemp in Peru.
1563 AD: English Queen Elizabeth I decrees that land owners with more than 60 acres must grow hemp or be fined 5 pounds.
1564 AD: King Philip of Spain orders hemp grown throughout his empire from modern Arhentina to Oregon.
1600 AD: Dutch achieve the “Golden Age” through hemp commerce. Explorers find “wilde hempe” in North America.
1606 AD: The British take cannabis to Canada for maritime uses.
1611 AD: The British start growing cannabis in Virginia.
1619 AD: Virginia colony makes hemp cultivation mandatory, followed by most other colonies. Europe pays hemp bounties.
1621 AD: Burton’s The Anatomy of Melancholy claims cannabis is a treatment for depression.
1631 AD: Hemp used as money throughout American colonies.
1632 AD: The Pilgrims take cannabis to New England.
1637 AD: The General Court at Hartford, Connecticut, orders that all families plant one teaspoon of cannabis seeds.
1639 AD: Massachusetts Courts follow Hartford.
1753 AD: Cannabis Sativa classified by Linneaus.
1763 AD: New English Dictionary says cannabis root applied to skin eases inflammation.
1776 AD: Declaration of Independence drafted on hemp paper.
1791 AD: President Washington sets duties on hemp to encourage domestic industry. “Make the most of the Indian Hemp Seed”….. Pres. George Washington, (Library of Congress).
1794 AD: Vol. 33 p.270). President Jefferson calls hemp a necessity and urges farmers to grow hemp instead of tobacco.
1800 AD: Cotton gins make cheaper fibre than hemp. Napoleon prohibits his men in Egypt from using cannabis, but to little effect.
1835 AD: The Club de Hashichines is founded.
1839 AD: Homeopathy journal ‘American Provers’ Union’ publishes first report on effects of cannabis.
1840 AD: “Prohibition… goes beyond the bounds of reason in that it attempts to control mans’ appetite through legislation and makes a crime out of things that are not even crimes… A prohibition law strikes a blow at the very principles upon which our Government was founded”…. Abraham Lincoln (December 1840).
1841 AD: Dr. W.B. O’Shaughnessy, “On the Preparation of the Indian Hemp or Ganja” introduces cannabis to western science.
1845 AD: Psychologist and inventor of modern psychopharmacology and psychotomimetic drug treatment, Jacques-Joseph Moreau de Tours documents physical and mental benefits of cannabis.
1850 AD: Petrochemical age begins. Toxic sulphite and chlorine processes make paper from trees: steamships replace (hemp) sails; tropical fibres introduced. USA census records 8327 hemp plantations of over 2000 acres each.
1854 AD: Bayard Taylor essay “Visions of Hashish”.
1857 AD: Fitz Hugh Ludlow publishes The Hasheesh Eater.
1858 AD: Smith Brothers of Edinburgh market cannabis indicia extracts.
1860 AD: First governmental commission study of cannabis and hashish conducted by Ohio State Medical Society. It catalogues the conditions for which cannabis is beneficial: neuralgia, nervous rheumatism, mania, whooping cough, asthma, chronic bronchitis, muscular spasms, epilepsy, infantile convulsions, palsy, uterine hemorrhage, dysmenorrhea, hysteria, alcohol withdrawal and loss of appetite.
1868 AD: The Emir of Egypt makes the possession of cannabis a capital offence.
1869 AD: Tales of Hashish by A.C. Kimmens.
1870 AD: Cannabis listed in US Pharmacopoeia as a medicine.
1870 AD: South Africa worried about cannabis use among Indian workers, passes a law forbidding the smoking, use or possession of hemp by Indians.
1876 AD: Hashish served at American Centennial Exposition.
1877 AD: The Sultan of Turkey makes cannabis illegal, to little effect.
1894 AD: British Indian Hemp Drugs Commission studies social use of cannabis and comes out firmly against its prohibition.
1895 AD: First known use of the name “marijuana” for smoking, by Pancho Villa’s supporters in Sonora, Mexico.
1909 AD: Shanghai Conference: First International meeting on drugs is held to discuss opium. The USA passes an act to prohibit the buying or selling of opium for non-medicinal purposes.
1910 AD: African-American “reefer” use reported in Jazz Clubs in New Orleans, said to be influencing white people & Mexicans smoking marijuana in Texas. South Africa prohibits cannabis.
1911 AD: Hindus reported to be using ganja in San Francisco.
1911 AD: South Africa bans cannabis.
1912 AD: “Essay on Hasheesh” by Victor Rolson. The possibilities of putting controls on cannabis use are first raised.
1912 AD: Hague Conference; second International meeting on drugs. 46 nations discuss opium, morphine, cocaine, heroin and cannabis. The Hague Convention for the Suppression of Opium and other drugs, was drawn up, requiring parties to confine to medical and legitimate purposes the manufacture, sale and use of opium, heroin, morphine and cocaine; Cannabis was not included. (From Mandeson, D. from Mr Sin to Mr Big, A History of Australian Drug Laws, Oxford University Press Melbourne, 1995).
1912 AD: First suggestions that cannabis should be banned internationally, at the First Opium Conference.
1915 AD: Utah State, then California and Texas outlaw cannabis. Cocaine banned in the USA.
1916 AD: USDA Bulletin 404 calls for a new program of expansion of hemp to replace uses of timber by industry.
1919 AD: Texas outlaws cannabis. Alcohol is prohibited throughout the USA. Cannabis is still legal in most States.
1920 AD: DuPont experiments with petrochemicals. Gang war takes over the alcohol industry, homicides increase drastically.
1923 AD: South African delegate at League of Nations calls for international controls on cannabis, claiming that it makes mine workers less active. Britain insists on further research.
1923 AD: Louisiana, Nevada, Oregon and Washington outlaw cannabis.
1924 AD: At the Second International Opiates conference Egyptian delegate claims serious problems are associated with hashish use and calls for immediate international controls. Sub-committee listens to Egypt and Turkey. Cannabis declared a narcotic. Cannabis Ruderalis identified by Lamarck.
1927 AD: New York outlaws cannabis.
1928 AD: UK Dangerous Drugs Act (September 28th) becomes law and makes cannabis illegal.
1929 AD: The Panama Canal Zone Report concludes that there is no evidence that cannabis use is habit forming or deleterious, recommending no action be taken against cannabis use or sale.
1929 AD: South West states make cannabis illegal as part of a move to oust Mexican immigrants.
1930 AD: Henry Ford makes his motor cars out of hemp with hemp paint and hemp fuel. New machines invented to break hemp, process the fiber and convert the pulp or herds into paper, plastics etc. 1200 hash bars in New York City. Racist fears of Mexicans, Asians and African-Americans fuel the cry for cannabis to be outlawed.
1930’s AD New mechanized hemp harvesting methods invented.
1930 AD: Louis Armstrong arrested in Los Angeles for possession of cannabis.
1931 AD: Federal Bureau of Narcotics formed with Anslinger as its Director. By now 29 US States have banned non-prescription cannabis.
1934 AD: Anslinger refers to “ginger-haired niggers” in FBI official circulars.
1936 AD: South Western states call for FBI to ban cannabis.
1937 AD: Marijuana Tax Act forbids hemp farming. The Act was based on the Machine Gun Transfer Act which made it illegal to pass on machine guns without a government stamp there being no such stamps available. By applying this strategy to marijuana, Anslinger was able to effectively ban hemp without contravening constitutional rights.
1937 AD: DuPont files patents for nylon, plastics and a new bleaching process for paper. Anslinger testifies to congress that Marijuana is the most violence causing drug known to man. The objections of the American Medical Association are ignored. The Marijuana Transfer Tax Bill (14th April) introduced to US House, Ways and Means Committee, passed December, prohibits industrial and medical uses and calls flowering tops a narcotic. Violations attract 200 dollar fines. Birdseed, rope and cordage are exempted from tax.
1937 AD: DuPont patents plastics, seizing the opportunity created by cannabis hemp prohibition.
1939 AD: LaGuardia Report started.
1941 AD: Cannabis dropped from USA Pharmacopoeia.
1941 AD: Henry Ford’s car is made from and runs on cannabis.
1943 AD: Hemp for Victory program urges farmers to grow hemp to help war effort.
1943 AD: US Military Surgeon magazine declares that smoking cannabis is no more harmful than smoking tobacco.
1944 AD: New York Academy of Medicine reports marijuana use does not cause violent behavior, provoke insanity, lead to addiction or promote opiate usage. Anslinger describes the authors as dangerous and strange.
1944 AD: New York Mayor’s La Guardia Report “The Marijuana problem in the City of New York” concludes that smoking marijuana does not lead to addiction in the medical sense of the word, that juvenile delinquency is not associated with marijuana smoking and that the publicity concerning the catastrophic effects of marijuana smoking in New York is unfounded.
1944 AD: Anslinger threatens doctors who carry out cannabis research with imprisonment.
1945 AD: USA ‘Newsweek’ reports over 100,000 Americans use cannabis.
1948 AD: Anslinger now says cannabis users are peaceful and that cannabis could be used during a communist invasion, to weaken American will to fight.
1948 AD: United Nation’s Universal Declaration of Human Rights
1948 AD: Hollywood star Robert Mitchum arrested for cannabis.
1951 AD: UN Bulletin of Narcotic Drugs states over 200 million cannabis users in the world.
1952 AD: First UK cannabis arrest at Number 11 Club, Soho, London.
1955 AD: Hemp farming outlawed again.
1960 AD: Hippies, Vietnam Veterans, pop fans adopt cannabis.
1961 AD: UN Treaty 406 Single Convention on Narcotic Drugs seeks to outlaw cannabis use and cannabis cultivation worldwide and eradicate cannabis smoking within 30 years (by 1991). USA representative is Anslinger.
1962 AD: President Kennedy sacks Anslinger. Kennedy is using cannabis as a pain relief.
1963 AD: Kennedy assassinated.
1964 AD: The Lin Brothers open first US ‘Head Shop’.
1964 AD: THC, Tetrahydrocannabinol, first isolated.
1966 AD: Donovan becomes first UK celebrity to be busted for cannabis.
1967 AD: SOMA Times Petition in the UK urges legalization of cannabis. The Beatles sign. 3,000 people hold a ‘smoke-in’ in Hyde Park. Keith Richards and Mick Jagger of the Rolling Stones are arrested and imprisoned for cannabis. This prompts a Times editorial ‘Who breaks a butterfly on a wheel’? The convictions are quashed on appeal. In the UK 2,393 persons are arrested for cannabis offences. In the USA, over 3,000 joints mailed to addresses at random by Abbie Hoffman and the Yippies.
1968 AD: John Lennon arrested for cannabis possession.
1968 AD: 1 November, 1968: UK Government Wootton Report recommends cannabis possession should not be an offence. “Having reviewed all the material available to us we find ourselves in agreement with the conclusion reached by the Indian Hemp Drugs Commission appointed by the Government of India (1893-94) and the New York Mayor’s Committee (1944 – LaGuardia) that the long-term consumption of cannabis in moderate doses has no harmful effects.”
1968 AD: Campaign to stop US soldiers in Vietnam from taking cannabis – The soldiers switch to heroin.
1969 AD: James Callaghan, UK Labor Prime Minister, rejects the findings of the Wootton Report.
1969 AD: Ex-Beatle George Harrison is arrested for cannabis.
1970 AD: Social use of cannabis receives widespread acceptance despite illegality; policy of decriminalization sweeps across USA and Britain.
1970 AD: LeDain Report (Canada) recommended that serious consideration be given to the legalization of personal possession of marijuana. It finds that cannabis use increases self-confidence, feelings of creativity and sensual awareness, facilitates concentration and self-acceptance, reduces tension, hostility and aggression and may produce psychological but not physical dependence. The report recommends that possession laws be repealed.
1970 AD: R. Keith Stroup founds NORML ‘National Organization for Reform of Marijuana Laws’, in USA.
1970 AD: USA Marijuana Transfer Tax declared unconstitutional.
1971 AD: British Misuse of Drugs Act classifies cannabis as a Class B drug with stiff sentencing. This bans the medical use of cannabis, ignoring the Wootton Report.
1971 AD: UN Convention on Psychotropic Substances.
1972 AD: US President Richard Nixon says ‘I am against legalizing marijuana’.
1972 AD: Baan Commission presents report to Dutch Minister of Health and suggests that cannabis trade below a quarter of a kilo ought to be considered as a misdemeanor only.
1973 AD: Oregon considering legalization.
1973 AD: US Shafer Commission, appointed by Nixon, declares that personal use of marijuana should be decriminalized as should casual distribution of small amounts for no or insignificant remuneration.
1973 AD: UN Convention of Psychotropic Substances: cannabis is a narcotic.
1974 AD: US Senate report on Marijuana- Hashish Epidemic and its Impact on US Security claims that cannabis use causes brain damage, a-motivation and genetic and reproductive defects.
1975 AD: Hundreds of US doctors call for more research on cannabis.
1975 AD: Alaska legalizes cannabis for personal use. Limit on amount is one ounce.
1975 AD: After 3 years of campaigning to abolish penal sanctions for the consumption of drugs, Pannella forces the police to arrest him, by smoking a joint in public.
1975 AD: Jamaica Studies reveal good health amongst prolific cannabis users. “No impairment of physiological, sensory and perceptual performance, tests of concept formation, abstracting ability, and cognitive style, and tests of memory”.
1976 AD: Holland adopts tolerant attitude to cannabis and many coffee shops and youth centers are allowed to sell cannabis.
1976 AD: USA New York Times (Jan 5) declares ‘Scientists find nothing really harmful about pot’.
1976 AD: Ford administration bans medical research on cannabis. Research on synthetic cannabis analogues continues. Robert Randal is the first US citizen to receive cannabis from Federal supplies made under the Investigational New Drug (IND) Program.
1976 AD: DuPont declares cannabis is less harmful than alcohol or tobacco and calls for its decriminalization.
1976 AD: USA President Ford bans medical research on cannabis.
1977 AD: President Carter thinks cannabis should be legalized.
1977 AD: The Australian Senate Standing Committee on Social Welfare (The Baume Committee) recommends treating drug use as a social/medical problem rather than legal problem. Also, that criminal sanction of possession of cannabis be replaced by fines while retaining penalties for possession of hashish, oil and purified THC.
1978 AD: State of New Mexico allows cannabis for sale for medical use, only.
1978 AD: The New South Wales Joint Parliamentary Committee upon Drugs recommends eliminating criminal sanctions for personal use of cannabis, implementing bond and probation penalties for first offenders and expunging records upon successful completion of these punishments. Also, suggest retaining penalties for trafficking in cannabis.
1980 AD: Ex-Beatle Paul McCartney arrested for cannabis and spends 10 days in prison in Japan.
1981 AD: Costa Rica study reports good health in cannabis users.
1982 AD: Coptic Study claims ‘No harm to human brain or intelligence’ with cannabis use.
1983 AD: In the UK over 20,000 convictions for possession of cannabis.
1984 AD: The USA government (Reagan/Bush) orders American Universities to destroy all the 1966-76 research work on cannabis.
1985 AD: Winters and DiFranza reveal radioactive material in tobacco may account for half the lung cancer deaths; No radioactive material ever detected in cannabis.
1986 AD: UK Drug Trafficking Offences Act introduced to enable confiscation of assets from drug dealers.
1987 AD: The USA Merck Manual of Diagnosis and Therapy says: “Cannabis can be used on an episodic or continual basis without evidence of social or psychic dysfunction. In many users the term dependence with its obvious connotations, probably is mis-applied… The chief opposition to the drug rests on a moral and political, and not toxicologic, foundation”.
1988 AD: 6 September: DEA Chief Administrative Law Judge, Judge Young, rules the US government should allow the medicinal use of cannabis. He says “Marijuana, in its natural form, is one of the safest therapeutically active substances known to man”. DEA rejects report.
1988 AD: 20 December: UN Convention against illicit traffic in narcotic and psychotropic substances, Vienna, includes cannabis.
1989 AD: Presidents Reagan and Bush declare war on cannabis; shops selling smoking apparatus are outlawed. Urine testing introduced & decriminalization, asset and property seizure, armed forces, prison camps, ‘Just Say No’ campaign, PFDA, DARE, tobacco and nuclear subsidies. Price -per-ounce of cannabis is worth more than gold. Worldwide prohibition entices organized crime to take control of the cannabis market and make huge profits. Reagan declares victory in War on Drugs. Secretary of State James A. Baker reports global war on narcotic production is ‘clearly not being won’.
1990 AD: Jack Herer, in his book ‘The Emperor Wears No Clothes’ offers $10,000 reward to anyone who can disprove his assertion that hemp can ‘save the planet’.
1990 AD: Alaska recriminalizes cannabis possession.
1990’s AD: USA voters pass regional measures to allow medicinal use of cannabis. Interest in this and other uses of hemp add new support to campaign for the legal right to social/recreational use of cannabis.
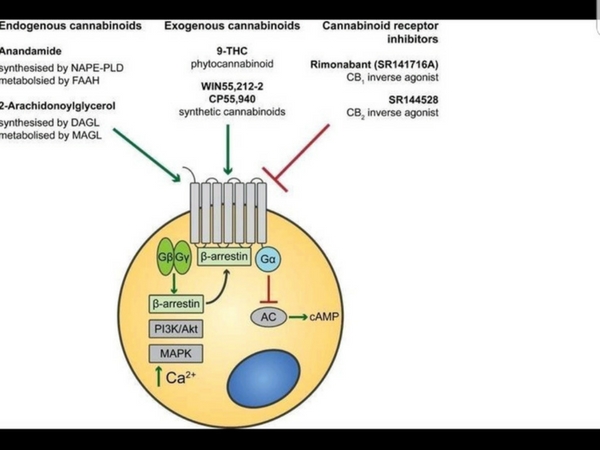
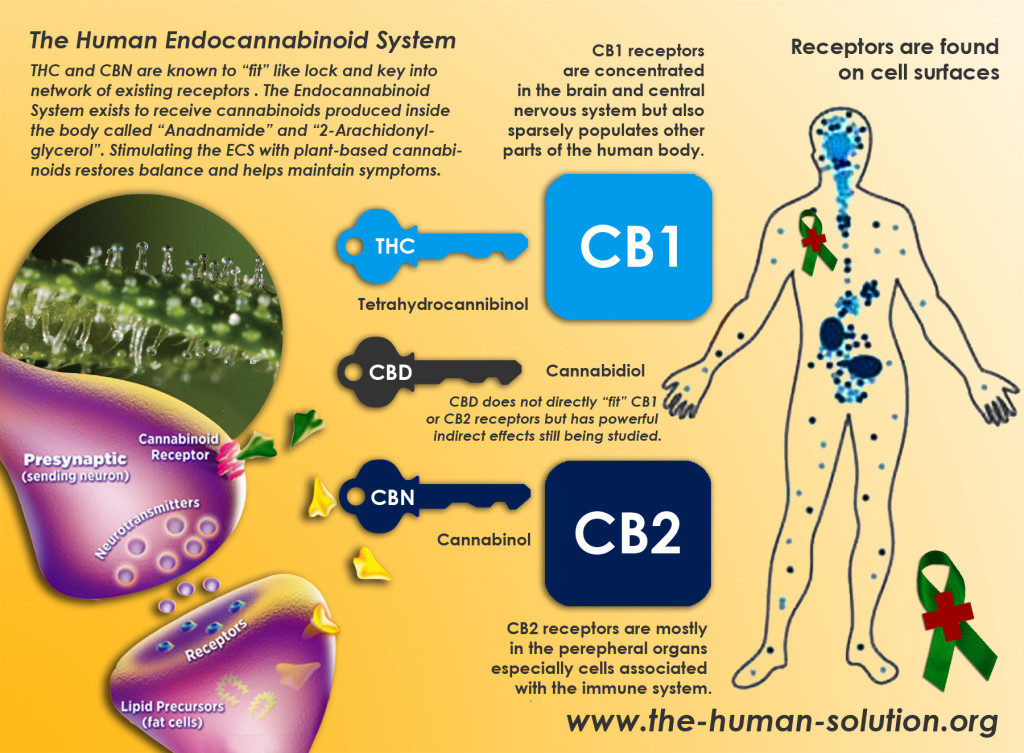
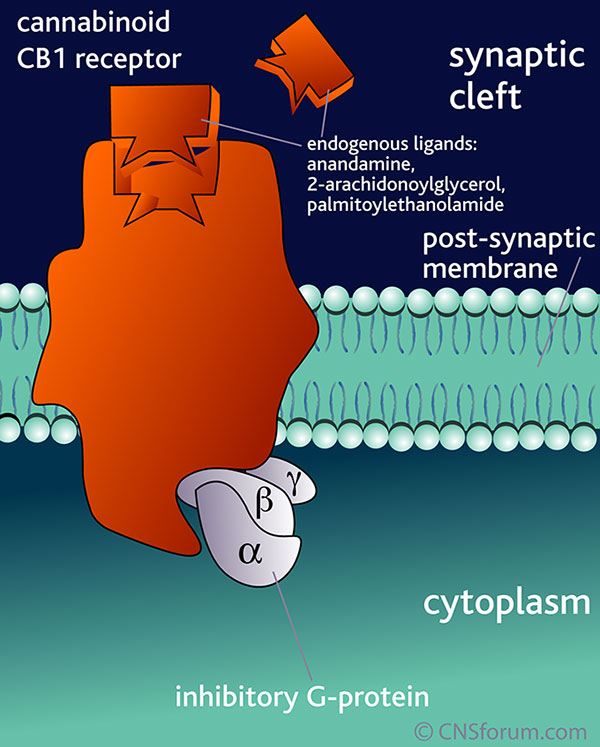
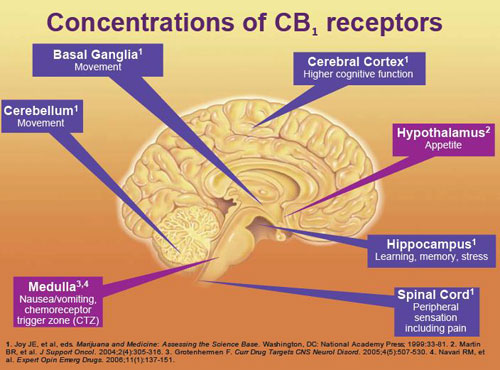
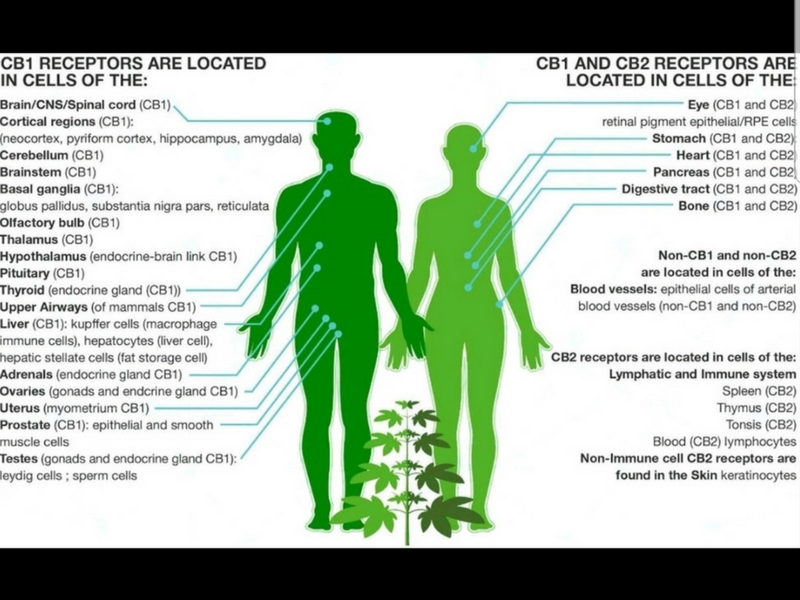
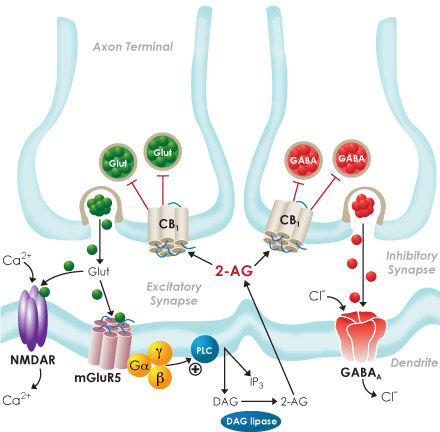
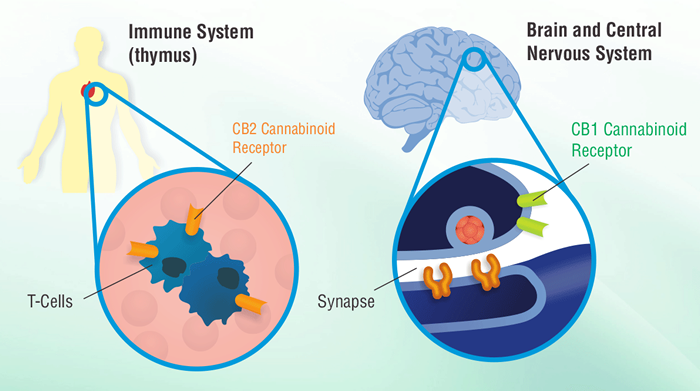
1991 AD: THC receptors found in the brain identified as CB1 & CB2 receptors.
1991 AD: In the UK over 40,000 people are arrested for cannabis.
1991 AD: ‘Mr. Marijuana’, Howard Marks, arrested, taken from Spain to USA and given 25 years imprisonment for trafficking in cannabis.
1991 AD: UK Judge Pickles advocates legalization of drugs.
1991 AD: UK PM Tony Banks (Labour Party) advocates for legalization of cannabis.
1991 AD: IND program dropped in USA.
1992 AD: January 22: California Research Advisory Panel reports that prohibition has a more harmful effect on society and the individual than illegal drugs themselves.
1992 AD: February 19: UK Government issue licenses to grow cannabis for industrial uses or scientific research.
1992 AD: “Medicines often produce side effects. Sometimes they are physically unpleasant. Cannabis too has discomforting side effects, but these are not physical they are political” … The Economist March 28th, 1992.
1992 AD: In the USA there are over 340,000 arrests for cannabis, nationwide.
1992 AD: Australia licenses hemp farm.
1992 AD: USA President Clinton admits he smoked cannabis but did not inhale. Howard Marks admits that he smoked cannabis but never exhaled.
1992 AD: 17 European Cities sign Frankfurt Charter agreeing to tolerate social use of cannabis.
1992 AD: USA Jim Montgomery, a paraplegic who smoked cannabis to relieve muscle spasm, busted for two ounces of marijuana in Oklahoma, arrested and sentenced to life plus 16 years.
1993 AD: Britain eases restrictions on hemp farming. Hemp core is first British company to get a license. Hemp clothes sold in High Street shops.
1993 AD: Commander John Grieve of the UK Metropolitan Police calls for decriminalization of cannabis.
1993 AD: Raymond Kendall, Head of Interpol, calls for decriminalization of cannabis.
1993 AD: British Law Lord, Lord Woolf calls for legalization of cannabis.
1993 AD: 22 British MP’s call for the establishment of a Royal Commission.
1993 AD: German High Court in Kruhe rules that cannabis prohibition is unconstitutional.
1993 AD: 55 British MP’s call for cannabis to be recognized and allowed for treatment of Multiple Sclerosis.
1993 AD: British Horne Secretary Michael Howard declares ‘War on drugs’ and increases maximum fine for possession of cannabis to £2,500.
1993 AD: Over 72,000 UK citizens arrested for cannabis offences.
1993 AD: Canada permits a hemp farm in Ontario province.
1995 AD: Holland lowers the amount one can possess without prosecution to 5 grams (from 30) as a result of powerful international pressures from neighboring countries.
1995 AD: UK Horne secretary Michael Howard increases penalties for cannabis offenses.
1995 AD: Clare Short MP (Labour Party) calls for a Royal Commission on Cannabis and is reprimanded by her party bosses.
1995 AD: European Cannabis Consumers’ Union founded in Amsterdam.
1995 AD: USA Dan Perron forms Cannabis Buyers Club to distribute cannabis to the sick.
1995 AD: The European Council which defines political guidelines, orders a study of drug legislation and practice in the Union.
1995 AD: September 16: First CHIC (Cannabis Hemp Information Club) conference in London.
1995 AD: Under the Clinton administration 1,450,751 people had been arrested for cannabis, 86% being for possession only.
1995 AD: November 11: British journal of the medical profession, The Lancet, states that ”The smoking of cannabis, even long term, is not harmful to health”.
1995 AD: Henrion Commission Report, the official French State Commission in charge of drug policy supports decriminalization of cannabis and calls for a two-year trial period of regulated retail trade in cannabis. The French Government rejects these proposals.
1996 AD: Victoria (Australia) State Council urge decriminalization of cannabis.
1996 AD: The Institute for the Study of Drug Dependence – Drug Notes – Cannabis 1996, p.8 says: “All that can be said definitely is that 1) Cannabis use generally precedes the use of other illegal drugs. 2) Cannabis use does not necessarily (or even usually) lead to the use of other illicit drugs.”
1996 AD: UK Janet Paraskeno, magistrate and director of National Youth Agency calls for ‘legalization and not decriminalization’.
1996 AD: The Parliament of Luxembourg passes a motion calling for a program ‘of common measures for the liberalization of cannabis and its derivatives’ along with Belgium and the Netherlands and the harmonization of drug laws in Benelux countries.
1996 AD: UK Cannabis Awareness Month (September) on 68th anniversary of the law.
1996 AD: Ireland announces their plans to use cannabis as fuel to replace the use of the dwindling supplies of peat.
1996 AD: Dutch town council at Delfzij decides to sell cannabis through their own coffee shop. They name the shop ‘Paradox’. Profits used to provide information campaigns against ‘soft drugs’ in Dutch schools. Meanwhile the Dutch close many coffee shops, bowing to pressures from Germany and France.
1996 AD: The Canton of Zurich calls for legalization of cannabis.
1996 AD: UK Crown Prosecution Service dropping cases of possession and cultivation against some ill people (MS) as ‘not in the public interest to proceed’.
1996 AD: California and Arizona pass Propositions allowing the use of cannabis in the treatment of certain illnesses, Clinton is re-elected and the FBI threaten Doctors with prosecution.
1996 AD: A Swiss man, Zimmermann, is given a life sentence in the Maldives, for importing three cannabis seeds, found in his luggage as he flew in from India.
1996 AD: Legalize Ganja Jamaica formed.
1996 AD: In the New Zealand general election the legalese cannabis candidate in Mittertond received 30% of the vote. Overall they received 1.4% of the votes, insufficient to gain a seat under proportional representation.
1996 AD: 100 Italian MP’s call for legalization of cannabis in Italy.
1996 AD: The Sunday Times, 1 December, says that out of 45 UK judges questioned 16 wanted to see cannabis legalized.
1996 AD: June: Scottish Nationalist conference votes to allow cultivation for personal use and research into medical uses of cannabis states “Relatively few adverse clinical effects from the chronic use of marijuana have been documented in humans. However, the criminalization of marijuana use may itself be a health hazard, since it may expose the users to violence and criminal activity.”
1997 AD: An 8-year study at the University of California at Los Angeles (UCLA) School of Medicine concluded that long-term smokers of cannabis do not experience a greater annual decline in lung functions than non-smokers. Researchers said: “Findings from the present long-term follow-up study of heavy, habitual marijuana smokers argue against the concept that the continuing heavy use of marijuana is a significant factor for the development of [chronic lung disease]” “No difference were noted between even quite heavy marijuana smoking and non-smoking of marijuana.” Volume 155 of the American Journal of Respiratory and Clinical Care Medicine 1997.
1997 AD: January 16: A court in Texas, USA, sentences medical marijuana user, William J. Foster to 93 years imprisonment for cultivation of one plant.
1997 AD: Two Swiss Cantons decide to legalize possession of cannabis in small amounts and ask the national Government to do the same.
1997 AD: The German State of Schlewig-Holstein legalize possession of up to 5 grams of cannabis.
1997 AD: After appeals for clemency from the Swiss Government and letters from CLCIA supporters, the Maldives releases Zimmermann, the man given life for three seeds.
1997 AD: In the USA a $2 million study to prove cannabis smoking can cause cancer fails and announces that it does not. The release of the report is delayed due to ‘lack of supplies’.
1997 AD: Paul Flynn MP introduces an early Day Motion calling on the Government to recognize the medicinal uses of cannabis and to make it available in tablet form, also congratulating the citizens of California and Arizona.
1997 AD: February 11: USA Federal Government Authorities, led by Barry R. McCaffrey, Director of National Drug Control Policy, resists the medical supply or cannabis in California and Arizona, threatening to prosecute Doctor’s who prescribe or supply cannabis.
1997 AD: The UK elects a new Labor Government and the Prime Minister, Tony Blair, says he will not legalize cannabis.
1997 AD: Scottish Rite (Church) comes out in favor of legalizing cannabis.
1997 AD: Rob Christopher, founder of CHIC – the Cannabis Hemp Information Club – in London, changes his name to Free Rob Cannabis and invites arrest by distributing cannabis cookies on the steps of the Department of Health in London. He is not arrested.
1997 AD: USA marines use helicopters to destroy marijuana crops in Hawaii despite objections from the people.
1997 AD: The Kaiser Permanente Study (USA) –”Marijuana Use and Mortality” April 1997 American Journal of Public Health concludes “Relatively few adverse clinical effects from the chronic use of marijuana have been documented in humans. However, the criminalization of marijuana use may itself be a health hazard, since it may expose the users to violence and criminal activity.”
1997 AD: Researchers at the University of California (UCLA) School of Medicine announced the results of an 8 – year study into the effects of long-term cannabis smoking on the lungs. In Volume 155 of the American Journal of Respiratory and Critical Care Medicine, Dr. D.P. Tashkin reported: “Findings from the present long-term, follow-up study of heavy, habitual marijuana smokers argue against the concept that continuing heavy use of marijuana is a significant risk factor for the development of [chronic lung disease … Neither the continuing nor the intermittent marijuana smokers exhibited any significantly different rates of decline in [lung function] ” as compared with those individuals who never smoked marijuana. Researchers added: “No differences were noted between even quite heavy marijuana smoking and nonsmoking of marijuana.”
1997 AD: The British Medical Association (BMA) recommends the provision of medicinal cannabis in the UK.
1997 AD: The Attorney General and Minister for Industrial Relations, Australia, JW Shaw QC MLC, announced the end of prison sentences for young cannabis offenders, saying that “I believe many parents would see the imprisonment of their son or daughter for using cannabis as particularly harmful.”
1997 AD: SYDNEY MORNING HERALD July 21 1997 p5 reports “A survey of a traditionally conservative NSW electorate has shown overwhelming community support for the decriminalization of cannabis.” New South Wales then decriminalizes possession of cannabis – up to 5 plants, 30 grams of leaf, 3 grams of resin and 2 grams of oil.
1997 AD: UK. After the shooting of a five year old boy in Bolton in a drug-related attack, Labor MP Brian Iddon calls for a Royal Commission on drugs with a view to decriminalization. The Sun conducts a poll that showed that over 40% of its readers are in favor of decriminalization. Labour Horne Office spokesman George Howarth says on Radio 4 News that cannabis causes harm and that Labor will never have dialogue on legalization and that the only solution is to stamp it out.
1997 AD: On September 19th, Marco Pannella is sentenced by the Rome Court to 4 months imprisonment commuted to 8 months on probation, for distributing hashish at the Porta Portese.
1997 AD: Sir Paul McCartney, ex-Beatle, reconfirms his call to decriminalize cannabis.
1997 AD: November 5: EU Parliament Committee on Civil Liberties suggests that soft drugs should be legalized.
1997 AD: December 3: The French secretary of State for Public Health, Bernard Kouchner, in favor of the supply of heroin to people suffering from severe heroin addiction. He also supports the medical application of cannabis, according to an interview with Dr Kouchner MD in the newspaper Liberation.
1997 AD: December 19th : DEA formally asked the Department of Health and Human Services to conduct “a scientific and medical evaluation of the available data and provide a scheduling recommendation” for marijuana and other cannabinoid drugs. This DEA request of HHS means that the DEA has for the first time made its own determination that sufficient grounds exist to remove marijuana from Schedule I of the Controlled Substances Act (CSA). Schedule I is supposed to be limited to hard drugs with addictive propensities and with no legitimate medical usage.
1998 AD: March: Madrid – European and American scientists defended medical marihuana at an International Symposium on Cannabis and the Brain held at the Fundacion Ramon Areces. According to them, the plant is effective in treating people with cancer and multiple sclerosis, but is not addictive.
1998 AD: Australia: March: Victoria’s police commissioner, Mr. Neil Comrie, has admitted the fight against drugs has failed and is set to introduce a radical statewide plan to keep drug users out of courts.
1998 AD: April: Czech Republic – President Vaclav Havel vetoes a law banning possession of drugs for personal use and sent it back to Parliament, citing human rights concerns. ‘The President reached the opinion that the law would lead to the prosecution of victims rather than culprits,” said spokesman Ladislav Spacek. Drug experts have warned that the legalization could lead to an increase in crime and drug prices and a decline in the willingness of addicts to be cured. – Reuters
1998 AD: 21 April, Belgium officially decriminalizes cannabis after a decision by Minister de Clerck of Justice. That is you will not be prosecuted for possession for personal consumption.
1998 AD: Italy decriminalizes possession of drugs and permits small scale cultivation of cannabis for own use.
1998 AD: June 12: The UK Government has granted a license to grow and possess cannabis for the purposes of medical trials, to Dr. Geoffrey Guy of GW Pharmaceuticals. The crop at a secret location in south-east England is guarded by electrified razor wire fences, security cameras and guard dogs.
1998 AD: Whilst US Federal Authorities make threats and arrests of Californian doctors who recommend cannabis and force the closure of most medical marijuana clubs in the state, Oakland City by-passes federal law by appointing medical marijuana suppliers as deputies thereby making them immune from arrest.
1998 AD: Germany: A petition of 30 thousand signatures organized by the “Selbsthilfegruppe Cannabis als Medizin” in Berlin was handed in to the Senat of Berlin in March 1998. All governing parties (CDU, SPD, PDS and Bundnis 90 / Die Grunen)discussed the issue and unanimously support it! The signatures being collected currently, will be handed to the “Petitionsausschuss des Deutschen Bundestages” together with the 30 thousand from Berlin .. ACM, Arbeitsgemeinschaft Cannabis als Medizin (Association for Cannabis as Medicine).
1998 AD: November 11: UK. The House of Lords rule that based upon the evidence presented for them the Government should make cannabis available to the sick without further delay, but that they are against legalization for recreational use. Jack Straw, Home Secretary, immediately rejects the House of Lord’s Report saying that cannabis will not be made available until a suitable pharmaceutical standard preparation has been thoroughly tested.
1998 AD: November: “We .. say that on the medical evidence available, moderate indulgence in cannabis has little ill-effect on health, and that decisions to ban or legalize cannabis should be based on other considerations.”: The Lancet, vol 352, number 9140, November 14, 1998.
1998 AD: December 24: Prince Charles tells a sufferer of Multiple Sclerosis that he has heard that cannabis can help.
1999 AD: January 21: USA: Medicinal Marijuana Advocate, Steve Kubby and Wife Busted.
1999 AD: March 4 : ALASKA: Medical Marijuana Law Starts.
1999 AD: March 23: GERMANY: Health Minister Supports Medical Marihuana
1999 AD: March 30: CANADA: Pot Users Take Fewer Road Risks Than Drunks Study Says.
1999 AD: April 1: USA: Farmers Lobby to Legalize the Growing of Hemp.
1999 AD: May 10: USA: NV Assembly Bill Eases Marijuana Penalties.
1999 AD: June 11: US Kentucky: Hemp Museum Opens Doors to History Of Versatile Plant.
1999 AD: June 13: UK: Cannabis Inhalers In First Legal Health Test.
1999 AD: June 21: CANADA: Compassion Club To Grow Pot in Homes of Members.
1999 AD: June 21: SCOTLAND: Doctors Back Legalizing Cannabis.
1999 AD: Oct. 14: Kingston, Jamaica: The Jamaican Senate has unanimously approved a resolution establishing a commission to explore the decriminalization of marijuana.
2000 AD: March 6: UK: First Conference of The Legalize Cannabis Alliance.
2000 AD: March 25: UK: Inquiry Calls For Softer Line On Hard Drugs – But Blair Says No.
2000 AD: March 29: SWITZERLAND: Swiss Parliament Legalizes Cannabis.
2000 AD: April 4: MALAWI: Minister Steps Up Campaign To Legalize Marijuana.
2000 AD: July 17: USA CA: Federal Judge Clears Way for Oakland Club to Distribute Pot to Seriously Ill Patients.
2000 AD: July 31: CANADA: Pot Prohibition Unconstitutional, Rules Court Of Appeals.
2000 AD: September 6: EUROPE: Dutch, Swiss and German Governments To Act on Marijuana
2000 AD: September 14: USA CA: Feds Rule Doctors May Recommend Pot.
2000 AD: October: Canadian Government Will Legalize Medical Marijuana Use
2001 AD: 19 January: BELGIUM: Seen Decriminalizing Cannabis Use.
2001 AD: 21 March: MEXICO: Leader Backs Call To Legalize Drugs.
2002 AD: August: Israeli Government Approves Use of Medical Marijuana/Cannabis by terminally ill.
2003 AD: February: US Jurors Become Angry that Trial Judge had not informed them that Ed Rosenthal was deputized by city authorities in Oakland, after they convicted him of cultivation.
2005 AD: April: “Marijuana is the equivalent of heroin and cocaine”. FDA issues statement denying that marijuana has any medical benefit.
2006 AD: December: California Compassionate Caregivers founded in Placentia, CA by Steele & Theresa Smith.
2006 AD: May: Mexican Congress passes bill legalizing all drugs for private personal use. The officially permitted quantities: up to five grams of marijuana; five grams of opium; 25mg of heroin; 500 mg of cocaine ; a few tabs of Ecstasy; small quantities of amphetamines and magic mushrooms; and up to a kilo of the sacred cactus peyote. Vicente Fox, Mexico’s President, pledges to sign the Bill – but capitulates to US government pressure 24 hours later. The bill is returned to Congress for revision.
2007 AD: April: Harvard university study shows that Delta-tetrahydrocannabinol (THC), the active ingredient in marijuana, cuts tumor growth in common lung cancer in half and significantly reduces the spread of cancer.
2007 AD: November 01: Activists Steele & Theresa Smith are indicted on Federal Cultivation charges; They face a 10 year minimum mandatory sentence for cultivating over 1,000 plants for their CA State legal collective named California Compassionate Caregivers. Their case becomes the first in US history where a Federal Judge allowed a medical defense in a Federal court when there is no such defense.
2008 AD: September 30: Steele Smith is released from Federal custody in LA pending trial; He is Innocent until proven guilty.
2009 AD: December: Greater Orange County Collectives Alliance (GOCCA.Org) Founded in Orange County, CA by Steele Clarke Smith, III.
2010 AD: November: CA state ballot scheduled on whether California should fully legalize marijuana, loses by 3% of vote.
2011 AD: Cannabis Industry Flourishes. Patents for Idrasil, the First Pure, Active Cannabis Pill are filed in US Patent Office.
2012 AD: May, the C3 Patients Association receives the first reimbursement for Idrasil from an Insurance company.
2012 AD: November, Colorado & Washington State all decriminalize the personal use of cannabis for up to one ounce.
2013 AD: New Hampshire legalized medical cannabis through the state legislature.
2014 AD: By the end of the year, ten more states followed Utah in legalizing low-THC, high-CBD cannabis oil: Alabama, Kentucky, Wisconsin, Mississippi, Tennessee, Iowa, South Carolina, Florida, North Carolina, and Missouri.
2015 AD: During the year, eight more states legalized low-THC, high-CBD cannabis oil: Delaware, Louisiana, Virginia, Georgia, Oklahoma, Texas, Delaware, and Wyoming.
2016 AD: Pennsylvania, Ohio, and Illinois decriminalized Medical Cannabis in the state legislature. Also, California, Nevada, Maine, and Massachusetts legalized recreational cannabis through a ballot measure.
2016 AD: Arkansas, Florida, and North Dakota legalized medical cannabis through a ballot measure.
2017 AD: Indiana legalized low-THC, high-CBD cannabis oil. West Virginia and New Hampshire decriminalized Cannabis in the state legislature. Indiana legalized low-THC, high-CBD cannabis oil.
2018 AD: Vermont became the first state to legalize recreational cannabis by way of state legislature.